

Comorbidity Factors (such as heart disease and diabetes) Influence COVID-19 Mortality More Than Age (Chapman University)
by Steven Gjerstad and Andrea Molle – Chapman University, USA
last update 2020.03.30
“It is an extremely important finding, not only because it allows for better decisions in the triage phase. But also because in the following phases, starting from the so-called phase 2 up to the production and distribution of a vaccine, it will be essential to make decisions aimed at protecting those who are the most at risk of serious consequences. Moreover, before the vaccine is distributed, individuals with hypertension, diabetes, heart disease, if not already developed immunity, will necessarily have to be closely monitored. Not only as they are at higher risk, but above all because if the disease is reactivating, we will see it in those with comorbidities, since healthy individuals tend to be asymptomatic and therefore could spread the virus silently.”
THE RESEARCH
The global reaction to the COVID-19 epidemic has rested on a critical assumption, that all persons over the age of 60 face an unacceptable risk of death if they are infected with the virus. Recent evidence from a detailed analysis of individual Chinese, American, and Italian patient data clearly indicates that this assumption is incorrect. Our research indicates that only 0.8% of all coronavirus-related deaths in Italy involved otherwise healthy individuals. The remaining 99.2% of deaths involved individuals who had at least one, and often at least 3 other illness factors. There are significant public policy implications to our quarantine and triage strategies.
Mortality from COVID-19 increases substantially with comorbidity factors, such as heart disease, hypertension, diabetes, stroke, and liver disease. After we control for the high incidence of comorbidity factors among the elderly, we find that mortality from coVid-19 does not vary much with age.
The coronavirus epidemic in Italy has strained hospital resources, including ICU beds and ventilators for those experiencing acute respiratory failure. Studies of COVID-19 in China [1], Italy [2], and the United States [3] show that fatality rates increase rapidly with age, especially beyond age 60. The same studies and others also show that fatalities increase substantially with comorbidity factors, such as heart disease, hypertension, diabetes, stroke, and liver disease [1, 4]. These morbidity factors are known to increase rapidly with age [5, 6, 7]. This paper demonstrates that once we control for comorbidity factors, age has a minor effect on COVID-19 mortality. Among the elderly the higher incidence of heart disease, diabetes, hypertension, and other comorbidity factors lead to their increased mortality form COVID-19. The distinction is an important one for the critical triage decisions that are required now. If it is the comorbidity factors that lead to death with COVID-19 patients and not age, then triage will be more effective if healthy elderly people are provided with treatment, since their chances of survival are good.
We examine 73,780 cases of COVID-19 and 6,801 deaths from COVID-19 in Italy through March 26, 2020. Based on estimates of the prevalence of comorbidity factors in Italy by age group and on the frequency of COVID-19 cases and mortality rates for age groups, we estimate the percentage of patients with and without morbidity factor that would be expected to die, first assuming that those with and without comorbidity factors are equally likely to die. Subsequently, we use a maximum likelihood estimate to get mortality probabilities for people in each age group, with and without comorbidity conditions. COVID-19 patients with comorbidity conditions are 10.5 times as likely to die than those without a comorbidity condition. For example, an Italian COVID-19 patient between 70 and 79 years old with no comorbidity factor has about a 1.6% chance of death, whereas a 70 to 79 year-old patient with a comorbidity condition has a 21.4% chance of death.
Triage decisions based on patient age do not account for the large differences between the prognosis for patients with and without morbidity factors. As medical resources become strained during the epidemic, it will be important to take account of the probabilities of survival for patients with different medical histories.
Analysis
Table 1 in [4] shows that 50.7% of the fatal cases of COVID-19 in Italy through March 26 had 3 or more of the comorbidity factors. Another 25.9% had 2 of these factors, and 21.3% had one factor. Only 2.1% had no factor. This last statistic is important. If age alone were an independent factor that leads to high mortality, then – we will demonstrate in this paper – there would be many more deaths among those who are elderly but otherwise healthy. In other words, the 2.1% frequency of no comorbidity factors would be much higher.
Tabella 1 in [8] shows that 19.2% of 73,780 COVID-19 cases in Italy through 4 p.m. on 26 March were among people age 70 to 79. From Tavola 7 in [7], we can infer that close to 25% of those people have none of the comorbidity conditions. We take death rates for the age groups from Tabella 1 in [8]. We consider the hypothesis that healthy people in each age group are as likely to die as those with 1 or more comorbidity condition. This hypothesis will lead us to the conclusion that there should be approximately 10.5 times as many people with no comorbidity factors as the number that are shown in Table 1 in [4].
People between 70 and 79 comprise 19.2% of the cases, and 25% of those have no comorbidity condition, so healthy people 70 – 79 years old are 4.8% of the cases. If healthy people between the ages of 70 and 79 are as susceptible to death from COVID-19 as those in their age group who have comorbidity conditions, then their death rate should be 16.9%, like their age group. If they were dying at the same rate as their age group, the fraction of all cases who would be people between 70 and 79 and have no comorbidity factor would be 0.048 x 0.1569 = 0.0081. Now we repeat this analysis for the remaining age groups and fill out Table 1.
Table 1: Column E shows the percentage of the 73,780 total cases that would be healthy people (i.e., no comorbidity factor) in their age group and would die from COVID-19.
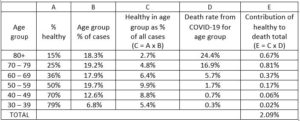
The total number of deaths that we would expect for people with no comorbidity factor would be this expected death frequency times the number of cases, which is 0.0209 x 73,780 = 1,542.
Table 2: Column E shows the percentage of the 73,780 cases in each age group that would die who have one or more comorbidity factor.
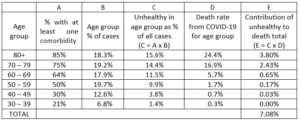
We now carry out a similar calculation in Table 2, but we consider here those people who have one or more comorbidity factor. This calculation shows that 7.08% of the total cases should be people with one or more comorbidity factor who died. That would result in 0.0708 x 73,780 = 5,223 deaths. As a check, total predicted deaths are 6,765. The total number of deaths from Tabella 1 in [8] where we get our total number of cases and our lethality factors for age groups (Column D) is 6,801.3
Our hypothesis that healthy people in each age group have the same probability of dying from COVID-19 leads us to the conclusion that of our estimated 6,765 deceased, 1,542 or 22.8% should have no comorbidity factor. Yet Tabella 1 in [4] shows that only 2.11% had no comorbidity factor. Consequently, the hypothesis that the probability of dying is the same for all people in an age group regardless of their comorbidity factors leads to the conclusion that there would be about 10.8 times as many deaths among those with no comorbidity factor than what we see in the sample of deceased persons in Tabella 1 in [4].
This analysis can be augmented by assuming different probabilities of mortality for those with and without comorbidity factors. If we multiply every element in Column D in Table 1 by 0.0925 we would get 143 deaths among those with no comorbidity factor. If we multiple every element in Column D, Table 2 by 1.2677 we would get 6,622 deaths among those with one or more comorbidity factor. We would then have 143/6,765 = 2.11% of the deceased having no comorbidity factor, as in Tabella 1 in [4]. The probabilities of death are then those in Table 3.
Table 3: These mortality probabilities produce fatalities in each age group that match total fatalities and match the frequency of comorbidities found in Tabella 1 in [4].
![]()
From this we conclude that age is most likely only a moderate factor leading to COVID-19 mortality. Of course, healthy elderly patients are not dying in large numbers from COVID-19, so triage decisions that ignore the elderly healthy are not likely to lead to large numbers of deaths within this group. These patients are likely to recover, but they are likely to recover more quickly and with less physical damage if they are provided treatment. They also are unlikely to require critical care for much longer than a healthy young person, since like the healthy young, they are recovering. For these reasons, we believe that triage decisions should be made without regard to a patient’s age.
About the authors
Steven Gjerstad, PhD, Economic Science Institute, Chapman University, 1 University Drive, Orange, California, 92866 USA, E-mail: gjerstad@chapman.edu; Tel: 714-628-7282
Andrea Molle, PhD, Institute for the Study of Religion, Economics and Society, Chapman University, Orange, California, 92866 USA
 per la sicurezza nazionale e la cooperazione regionale")






































There are no comments
Add yours